
On July 23-24, 2026, the FDA's Pharmacy Compounding Advisory Committee (PCAC) will convene at the White Oak Campus in Silver Spring, Maryland to evaluate whether several high-profile peptides — including BPC-157, TB-500, KPV, and MOTS-c — should be added to the 503A Bulks List . For providers who have been watching the regulatory landscape closely, this meeting represents a meaningful step forward.
But here is the question that most providers aren't asking yet: What if you want to offer peptides beyond the scope of what the FDA approves — without getting into trouble?
Because even if every peptide on the July agenda gets approved, the honest answer is that the 503A framework still won't give providers what they actually need.
What the FDA Meeting Actually Decides
To understand the ceiling of this meeting's impact, it helps to understand exactly what the PCAC is evaluating. The committee is not approving peptides for broad clinical use. It is evaluating whether specific bulk drug substances can be compounded by 503A pharmacies for very specific, FDA-reviewed indications.
Here is what is on the table:
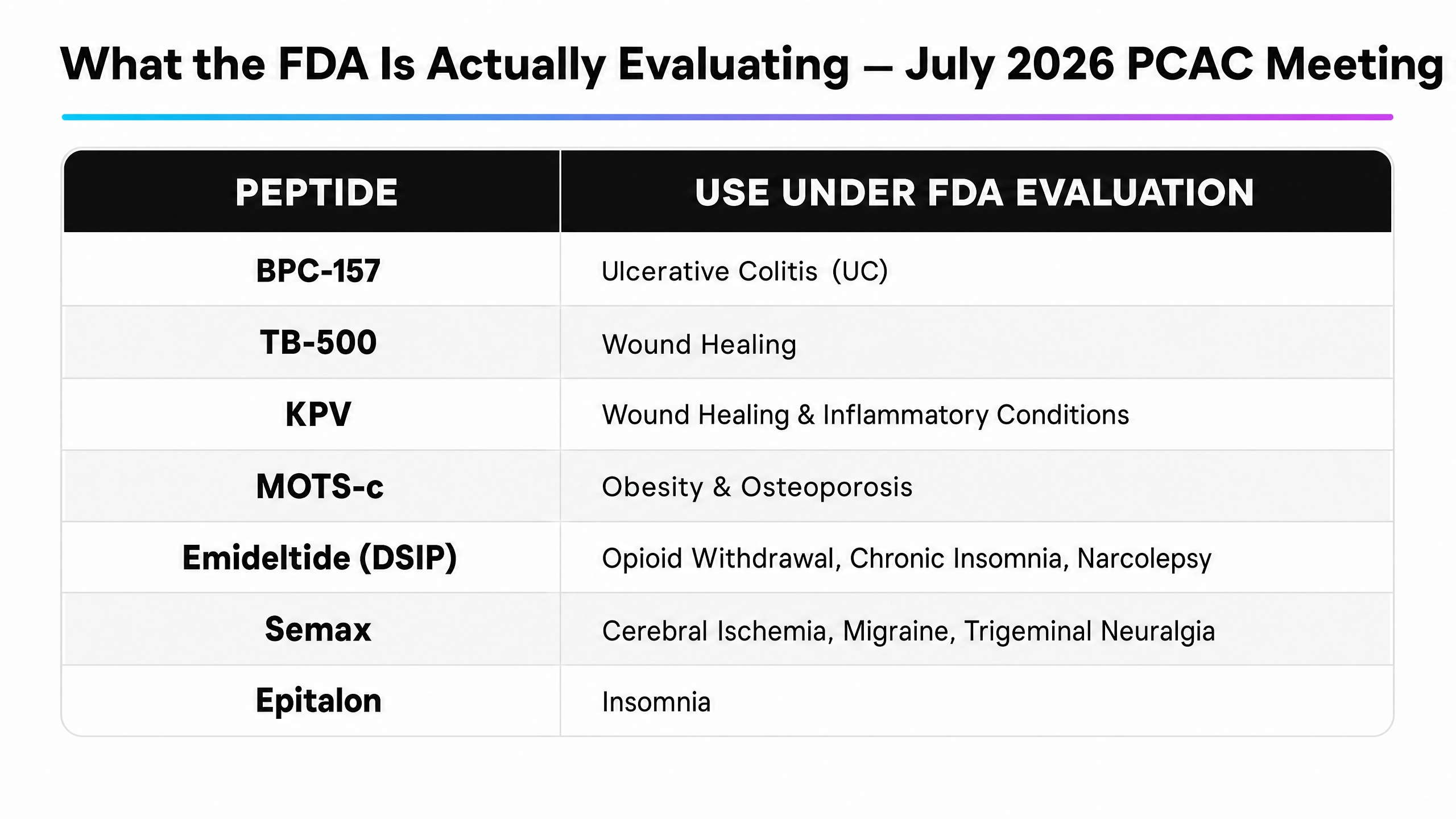
This is important to sit with. If BPC-157 is approved to the 503A list for Ulcerative Colitis, a compounding pharmacy is authorized to compound it for that indication. It does not mean a provider can prescribe it for musculoskeletal recovery, joint health, or general tissue repair — the very reasons most clients seek it out.
If a client wants to use BPC-157 and TB-500 together for recovery and mobility, the 503A framework almost certainly cannot support that combination, because BPC-157 would be evaluated for UC and TB-500 for wound healing. They are approved for different, narrow indications. Combining them for a broader wellness purpose falls entirely outside the compounding framework.
The Indication Trap: Why Approval Isn't Access
Section 503A of the Federal Food, Drug, and Cosmetic Act is explicit: compounders cannot compound drugs that are "essentially copies" of FDA-approved drugs, and compounding must be tied to a specific, individualized medical need that cannot be met by a commercially available product . This means the prescribing model requires:
A formal diagnosis that maps to an FDA-recognized indication. A documented medical necessity. A patient-specific prescription from a licensed provider.
For providers whose clients are seeking peptides for longevity, proactive recovery, metabolic optimization, or general wellness, none of these boxes can be checked. These are not disease states. They are not FDA-recognized indications. And prescribing compounded peptides for these purposes — even after the July meeting — would still place a provider's medical license in a precarious position.
The 503A approval process is a net positive for the peptide space. But it is not a solution for providers who want to offer peptides broadly and safely.
A Different Domain Entirely
What if the answer isn't to find a better path through the FDA's framework — but to operate in a domain where that framework doesn't apply?
Nuri conducts human research protocols involving investigational peptide therapies under the oversight of a privately funded university partner. This places Nuri's operations in the private, ecclesiastic research domain — not the public medical domain governed by FDA compounding rules or federal health care program statutes.
Because Nuri does not submit claims, seek reimbursement, or participate in any Federal health care program, the statutory triggers for both the Anti-Kickback Statute and Stark Law are absent. The AKS is expressly limited to conduct involving items or services reimbursable by a Federal health care program. Nuri's research protocols are privately funded and categorically excluded from federal reimbursement. Stark Law prohibits referrals to entities providing designated health services — and Nuri's private, at-home research protocols are not a designated health service, or a medical treatment in any way, shape, or form.
As a result, when a provider educates a client about the current peptide landscape and directs them toward Nuri's research programs, that referral activity does not fall within the scope of §1320a-7b or §1395nn. Any compensation a provider receives is derived solely from private, non-federal funds and is not connected to services reimbursable by federal programs — a distinction that courts have repeatedly recognized as placing purely private-pay referral arrangements outside the reach of these statutes.
What This Means for Providers in Practice
The July 2026 FDA meeting is meaningful. It signals a regulatory environment that is slowly warming to peptides, and 503A approval for even a handful of compounds is a step in the right direction for the broader industry.
But for a provider who wants to offer BPC-157 and TB-500 together for recovery, or MOTS-c for metabolic health beyond the narrow obesity indication, or Epitalon for longevity rather than insomnia — the 503A framework still cannot get them there. And the prescribing model still carries the license risk, the medical necessity burden, and the Anti-Kickback exposure that make it untenable for most practices.
Nuri's private research structure resolves all of these constraints simultaneously. Providers can educate their clients about investigational peptides, refer them into a structured, purity-tested research program, and receive compensation for doing so — all without writing a single prescription, without touching the compounding pharmacy system, and without exposure to federal health care fraud statutes.
The FDA meeting is good news. But it is not the answer to the question providers actually need answered.
References
Disclaimer
Programs and products offered through Nuri are not FDA approved and are provided as part of a structured wellness research program conducted under the oversight of a privately funded university partner. Participation does not constitute medical treatment, and no prescriptions are issued. Individual experiences may vary. Always consult a licensed healthcare professional before beginning any new wellness program.